It was clear from the beginning of data collection that stigma was significant to participants. The overall process described by participants co-created from the data as “Working Through Stigma”. Participants were aware of the impact of stigma on how health services are delivered to 2SLGBTQ populations within primary care settings in Nova Scotia and findings demonstrate the scale of stigma that individuals are working through. Participants who were 2SLGBTQ-identified experienced stigma differently than those who were non-2SLGBTQ identified; the impact depended on various factors that were explored through different aspects of identity. All participants described ways of negotiating power relations (by) working through stigma. HSPs stated intentions to avoid reproducing negative constructions in their individual practice, but there was evidence of power relations working through stigma in ways that were often beyond the control of individuals.
Working Through Stigma depicts the negotiation of power relations impacting the delivery of health services to diverse 2SLGBTQ populations in Nova Scotia. Findings illustrate that power works through stigma at intrapersonal, interpersonal, and contextual levels within primary care settings in Nova Scotia and shapes the conditions under which health services are delivered to 2SLGBTQ populations in ways that influence health outcomes. Stigma impacted HSPs in addition to HSUs, which suggests that more work needs to be done to diminish barriers to delivering and accessing health services. These barriers require active and intentional intervention to disrupt power relations that overlap and converge upon individuals by way of social categories of identity. If an HSP is not actively working through stigma, this means their share of the work falls upon the HSU and highlights the inequities that exist in health care and why underservicing of historically underrepresented groups persists. The ways that barriers are overcome to resolve the discrepancies between what is needed versus what is attainable depends on context; “how” stigma is (and can be) worked through is a complex process that is informed by ongoing and interacting personal and collective histories. The learning experiences of HSP and care recipient experiences of HSU participants reveal various ways that power relations work through stigma and highlight an opportunity to transform how health services are delivered to diverse 2SLGBTQ populations in Nova Scotia. Positive change could thus be supported within the primary care system if health-related education and institutional structures, systems, processes, and decision-making influenced the conditions under which health services were delivered by working through stigma in ways that disrupt, challenge, and transform power relations, rather than reproducing them.
Theory that challenges the very meaning of stigma was co-created. Participants in this study described ways of working through stigma that were often, but not always negative on impact, which invited a consideration of stigma's inherent negativity. Stigma is in every culture and it is used as a resource by dominant groups to uphold cultural supremacies by attributing negative meaning to arbitrary differences. What if stigma was used differently? The co-created theory accounts for the negative impacts of stigma, but it provides an alternate way of working through stigma that would anticipate the negative impacts in ways that would be equitable on impact. Essentially, this study generated theoretical knowledge that questions the meaning of stigma in ways that challenges negative constructions that uphold cultural supremacies.
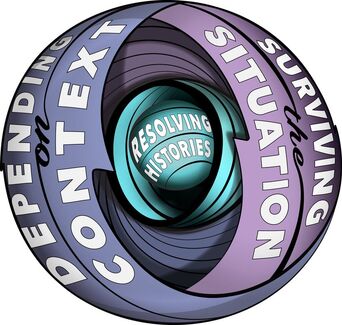
When working through stigma, everything depends upon the situatedness of individuals and the relationships they have with(in) society. Identity is a means by which power relations can work through stigma, but through resolving histories, individuals can work through stigma in ways that appreciate the ongoing and accumulating processes by which interactions between individuals in various contexts take place. As such, working through stigma is an opportunity for change to come about in primary care (and perhaps broader social contexts), and a means by which the relationship between stigmatized populations and the health system can be healed. The diagram below is a representation of the substantive theory on Working Through Stigma, grounded in the data collected in this study. It shows the three concepts feeding into and mutually constituting each other and represents a theoretical understanding of the ongoing social processes that reproduce hegemonic power relations, which can be challenged, disrupted, and transformed by intervening upon stigma within the context of primary care in Nova Scotia in ways that change the conditions under which health services are delivered.
Working Through Stigma depicts the negotiation of power relations impacting the delivery of health services to diverse 2SLGBTQ populations in Nova Scotia. Findings illustrate that power works through stigma at intrapersonal, interpersonal, and contextual levels within primary care settings in Nova Scotia and shapes the conditions under which health services are delivered to 2SLGBTQ populations in ways that influence health outcomes. Stigma impacted HSPs in addition to HSUs, which suggests that more work needs to be done to diminish barriers to delivering and accessing health services. These barriers require active and intentional intervention to disrupt power relations that overlap and converge upon individuals by way of social categories of identity. If an HSP is not actively working through stigma, this means their share of the work falls upon the HSU and highlights the inequities that exist in health care and why underservicing of historically underrepresented groups persists. The ways that barriers are overcome to resolve the discrepancies between what is needed versus what is attainable depends on context; “how” stigma is (and can be) worked through is a complex process that is informed by ongoing and interacting personal and collective histories. The learning experiences of HSP and care recipient experiences of HSU participants reveal various ways that power relations work through stigma and highlight an opportunity to transform how health services are delivered to diverse 2SLGBTQ populations in Nova Scotia. Positive change could thus be supported within the primary care system if health-related education and institutional structures, systems, processes, and decision-making influenced the conditions under which health services were delivered by working through stigma in ways that disrupt, challenge, and transform power relations, rather than reproducing them.
Theory that challenges the very meaning of stigma was co-created. Participants in this study described ways of working through stigma that were often, but not always negative on impact, which invited a consideration of stigma's inherent negativity. Stigma is in every culture and it is used as a resource by dominant groups to uphold cultural supremacies by attributing negative meaning to arbitrary differences. What if stigma was used differently? The co-created theory accounts for the negative impacts of stigma, but it provides an alternate way of working through stigma that would anticipate the negative impacts in ways that would be equitable on impact. Essentially, this study generated theoretical knowledge that questions the meaning of stigma in ways that challenges negative constructions that uphold cultural supremacies.
When working through stigma, everything depends upon the situatedness of individuals and the relationships they have with(in) society. Identity is a means by which power relations can work through stigma, but through resolving histories, individuals can work through stigma in ways that appreciate the ongoing and accumulating processes by which interactions between individuals in various contexts take place. As such, working through stigma is an opportunity for change to come about in primary care (and perhaps broader social contexts), and a means by which the relationship between stigmatized populations and the health system can be healed. The diagram below is a representation of the substantive theory on Working Through Stigma, grounded in the data collected in this study. It shows the three concepts feeding into and mutually constituting each other and represents a theoretical understanding of the ongoing social processes that reproduce hegemonic power relations, which can be challenged, disrupted, and transformed by intervening upon stigma within the context of primary care in Nova Scotia in ways that change the conditions under which health services are delivered.